




At Mongbwalu Hospital, the primary healthcare facility serving the mining town of Mongbwalu in Ituri Province, the realities of the Democratic Republic of Congo’s latest Ebola outbreak are unfolding in stark and often heartbreaking ways.
Inside a cramped treatment ward, a severely ill adult patient lay under observation. Nearby was a young child suspected of carrying the virus. In the same confined space rested the body of a patient who had already succumbed to the disease. For overstretched medical workers, it is a grim reflection of a health system struggling to keep pace with what has become one of the most serious Ebola emergencies in recent years.
The outbreak was first detected in the Mongbwalu Health Zone. The World Health Organization says health authorities were alerted on May 5 to an unknown illness with an unusually high mortality rate in Ituri Province, including the deaths of four health workers within days.
Laboratory tests later confirmed the outbreak as the Bundibugyo strain of Ebola, a rare variant for which there is currently no licensed vaccine or approved treatment.
The hospital itself reflects the wider fragility of Congo’s healthcare system. Far from a specialized Ebola treatment centre, Mongbwalu Hospital consists of modest brick buildings with aging corrugated iron roofs, limited isolation infrastructure and overstretched staff.
Families often bring food and water to relatives because the facility lacks the resources to provide even the most basic necessities.
Among the patients was a five-year-old boy whose father works as a motorcycle taxi driver in the town. After developing a fever and being sent home from school, the child was treated at home until his condition deteriorated dramatically. By the time he arrived at the hospital, he had begun bleeding heavily from the nose, one of Ebola’s most feared symptoms.
Doctors say delays in testing continue to complicate the response. Suspected cases are frequently housed alongside confirmed patients while awaiting laboratory results, increasing both fear and the risk of transmission.
The frustration is palpable among frontline health workers. One Congolese doctor questioned why it had taken so long for authorities and the international community to identify the outbreak and mobilize resources.
WHO figures show that, as of late May, the Democratic Republic of Congo had recorded 906 suspected cases and 223 suspected deaths. Across Congo and Uganda combined, 134 laboratory-confirmed cases and 18 confirmed deaths had been reported.
Ituri Province alone accounts for 88 percent of all confirmed infections, with Bunia reporting 37 confirmed cases, Rwampara 33, Mongbwalu 20 and Nyankunde 10. Authorities have identified more than 2,635 contacts requiring follow-up, while hundreds of samples have been collected for testing.
Ebola is transmitted through direct contact with the blood, bodily fluids or tissues of an infected person or animal, as well as contaminated materials such as clothing, bedding and medical equipment. The virus can also spread through contact with the bodies of deceased victims during burial ceremonies.
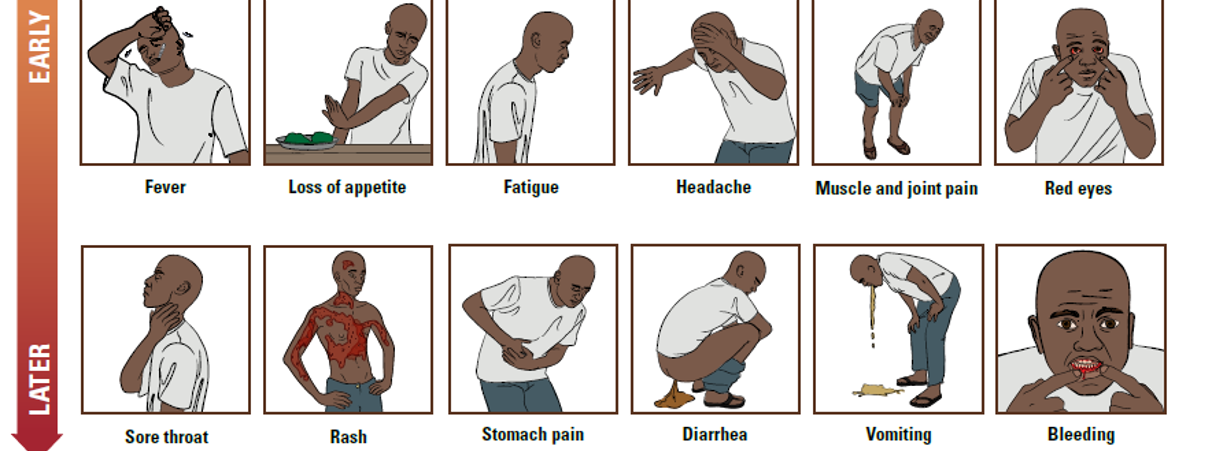
Symptoms often begin with fever, severe weakness, headaches and muscle pain before progressing to vomiting, diarrhoea, abdominal pain and, in severe cases, internal and external bleeding.

The outbreak has once again exposed the fragility of Congo’s healthcare system. Years of armed conflict, weak surveillance networks, chronic underinvestment and recurring humanitarian crises have left health authorities struggling to respond effectively. More than 273,000 people have been displaced in Ituri Province alone, while nearly 1.9 million require humanitarian assistance.
The crisis has also exposed longstanding weaknesses within the Congolese state. In many affected communities, particularly in parts of Ituri, the government’s presence is limited and response efforts depend heavily on underpaid health workers, volunteers, community leaders and humanitarian organizations.
Many frontline workers operate with limited protective equipment, inadequate transport and irregular salaries. In some areas, communities encounter volunteers, aid workers and local responders more frequently than representatives of the state itself.


The situation is not uniform across eastern Congo. While Ituri remains the epicentre of the outbreak, health authorities have also recorded cases in North Kivu Province. Public health workers note that some areas under the control of the M23 administration appear comparatively more organized and resourced in their response efforts.
Local authorities have conducted public awareness campaigns, community engagement activities, testing initiatives and hygiene measures aimed at reducing transmission risks. The M23 leadership has publicly urged residents to report symptoms early, comply with health guidance and cooperate with medical teams.
Health workers say that, despite ongoing challenges, the level of local mobilization and public engagement in some North Kivu communities has strengthened surveillance and preparedness efforts.
The outbreak has already crossed borders. Health officials in Uganda have confirmed cases linked to travel from eastern Congo, underscoring the risks posed by the region’s highly mobile population.
The crisis has also reached Europe. International health authorities report that an American healthcare worker infected while treating patients in Congo was transferred to Germany for specialized care.
European governments have since heightened surveillance measures while monitoring potential exposure risks linked to international travel from affected areas.
The worsening outbreak has prompted visits by senior global health officials. WHO Director-General Dr. Tedros Adhanom Ghebreyesus recently traveled to Bunia, the capital of Ituri Province, where he inaugurated a new Ebola treatment centre and met patients who successfully recovered from the disease.
WHO reports that several patients have now recovered and been discharged despite the absence of a dedicated vaccine.
Funding, however, remains a major concern. Africa CDC estimates that hundreds of millions of dollars are required to sustain the response, yet available resources remain significantly below operational needs.
Health officials warn that shortages of protective equipment, treatment facilities, laboratory capacity and medical personnel continue to undermine containment efforts.
The outbreak has also triggered international preparedness measures. Reports indicate that the United States and Kenya have expanded cooperation on Ebola preparedness, including plans for treatment and quarantine facilities designed to manage potential cases and protect regional and international health security.
Closer to the epicentre, Rwanda has adopted some of the region’s most stringent preventive measures. The Ministry of Health has strengthened screening and surveillance at all official border crossings, airports and points of entry.
Health teams have been deployed on heightened alert, emergency response systems activated and isolation facilities prepared across the country.
Rwanda has also imposed temporary restrictions on foreign nationals who have recently traveled through the Democratic Republic of Congo. Rwandan citizens and legal residents returning from Congo are subject to enhanced screening, mandatory monitoring and additional public health measures where necessary.
Authorities have emphasized that the measures are precautionary and intended to prevent the virus from gaining a foothold in the country.
Yet the battle against Ebola extends far beyond hospitals and border controls.
Images emerging from Ituri Province, the epicentre of the outbreak, reveal another challenge threatening containment efforts: community resistance fueled by misinformation and distrust.
In one incident, residents confronted teams conducting dignified and secure burials, a critical measure in preventing Ebola transmission. Witnesses reported that villagers threatened burial workers, seized a coffin, opened a body bag and handled the deceased’s body.
If the deceased was indeed a confirmed Ebola victim, such actions could significantly increase the risk of transmission. Ebola remains highly infectious after death, making safe burials one of the most important tools for breaking chains of infection.

The scenes illustrate how misinformation can undermine public health efforts. Health officials warn that rumours circulating through communities and social media have fueled suspicion toward medical workers, treatment centres and burial protocols, creating obstacles that no amount of medicine alone can overcome.
For families gathered outside Mongbwalu Hospital, however, the crisis is measured less in statistics than in uncertainty. Behind every suspected case is a child fighting a fever, a parent awaiting test results or a healthcare worker trying to save lives with limited supplies.
In places like Mongbwalu, Ebola is not merely a public health emergency. It is a daily struggle fought in overcrowded wards, under-resourced hospitals and communities where defeating the virus may ultimately depend as much on rebuilding trust as on delivering medicine.


{kind=link}